How To Tell If Someone Is Hoarding – and Provide Effective Help
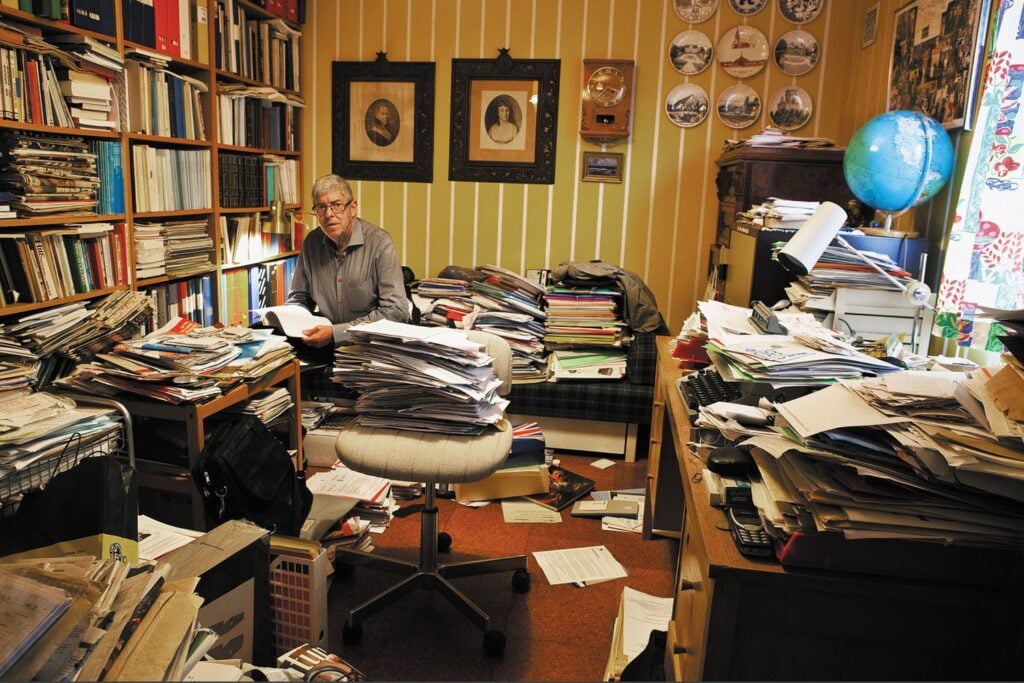
For many, letting go of possessions is intensely stressful, even when the clutter puts them at risk. Here’s what you can do Some messiness is a fact of life for most people. It might be piles of disorganised paper, a box of decades-old cheques, or dirty clothing strewn about a bedroom. Then there’s the mess behind closed doors – in closets and drawers, the attic, or the garage. Messiness is an index of where people are in life. As we age, or when we’re going through a difficult time, our living spaces may get cluttered because we just don’t have the stamina or strength to manage it. In certain cases, however, messiness sends an important signal about someone’s mental health. You might walk into the home of a friend or family member and find old or dirty items in every room, stacks of things that obstruct your movement, or storage areas that seem troublingly overstuffed. If you have noticed at some point that a person you care about has a severe problem with messiness, it makes sense to wonder if there’s something deeper going on. You’ve probably heard of hoarding disorder (HD), a psychological condition that is characterised by persistent difficulty with discarding possessions. People with this condition – which is estimated to affect around 1 in 50 adults – feel a need to save possessions regardless of their actual value, and they experience intense distress about letting go of these possessions. Over time, this leads to an accumulation of things, and a person’s living environment can become so highly cluttered that living there becomes challenging and even unsafe. Read the Full Article
Cognitive Behavioral Therapy for Depression
Dr. Monique Thompson’s newest book Cognitive Behavioral Therapy for Depression: Essential Strategies to Manage Negative Thoughts and Start Living Your Life was released on November 3, 2020. The book is designed to help people struggling with depression to discover the help they need to manage negative thought patterns and reconnect with their lives. Editorial Reviews Monique Thompson’s cogent and ultra-compelling book is simply the clearest, easiest-to-follow, and simultaneously deepest guide to Cognitive Behavioral Therapy for Depression I’ve ever read. Super-clear, with excellent clinical examples embedded in each chapter. Rather than learning high-level, abstract principles, the reader comes away with a real sense of what this evidence-based form of therapy looks like and feels like from the patient’s perspective. Highest recommendation–for clients, therapists-in-training, and the general public. — Steven Hinshaw, Professor of Psychology, UC Berkeley; Professor of Psychiatry, UC San Francisco, Author Another Kind of Madness “Cognitive Behavioral Therapy for Depression is a terrific resource for anyone suffering with depression and for therapists working to help them. Dr. Monique Thompson presents the principles and skills of cognitive behavior therapy clearly and compassionately. I highly recommend this book to anyone and everyone!” ―Michael A. Tompkins, PhD, Co-Director of the San Francisco Bay Area Center for Cognitive Therapy and Author of Anxiety and Avoidance: A Universal Treatment for Anxiety, Panic, and Fear “We find ourselves in complex and challenging times that can, for many, provoke an episode of depression. Fortunately, Monique Thompson’s Cognitive Behavioral Therapy for Depression has arrived as a practical, accessible, and science-based guide to understanding and conquering depression. It is full of real-life examples of the thoughts, feelings, and actions that combine to produce depression as well as essential strategies for taking action against these forces. Readers will be able to apply the lessons and strategies to their own lives, thanks to the clarity and compassion in Thompson’s prose. Whether used as a stand-alone guide or as a complement to therapy, this book is bound to help scores of people who deal with the all-too-common experience of depression.” ―Ann M. Kring, Ph.D., Professor, Department of Psychology, University of California, Berkeley “For those dealing with depression, personally or professionally, this is THE book to read! Beautifully written with clarity and precision, and grounded in empirically established methods, Monique Thompson provides a superb map and guidebook for navigating the terrain of depression and emerging in a much better place.” ―David E. Presti, Professor of Neurobiology, University of California, Berkeley and Author of Foundational Concepts in Neuroscience: A Brain-Mind Odyssey “This book offers, in a deceptively small package, a large collection of strategies the reader can act on now to overcome pessimism, hopelessness, guilt, and lethargy in order to dig out of the black pit of depression and despair. The author’s wise advice is based on both her personal experience of depression and her professional experience doing research on depression and providing treatment for it. Dr. Thompson’s writing is clear and direct, and she speaks with a warm and compassionate voice that is simultaneously solidly grounded in the latest science.” ―Jacqueline B. Persons, Ph.D., Director, Oakland Cognitive Behavior Therapy Center, and Clinical Professor, Department of Psychology, University of California, Berkeley
Five Spring Decluttering Tips

Develop a system to manage paper. Paper is the number ONE item when it comes to clutter. Newspapers, magazines, and junk mail all add to the mountain of paper in our homes. The first step in organizing paper is to develop a system to manage it. Think in terms of time. Papers such as the titles to your home and car you’ll likely keep until you sell them. Other items, such as a daily newspaper, you’ll keep until you recycle them: usually once each week. Some pieces of paper you can toss when you receive them, such as junk mail or an ATM receipt. So, create files and boxes organized by how long it makes sense to keep a piece of paper. For example, a “Until Sold” box or file might hold the title to your car. You might create a “One Year” box or folder to keep your home and car insurance policies (which is the usual renewal period). Sort first. Once you’ve created systems to store paper and other possessions, the next step is to sort your possessions into categories. It’s impossible to declutter your living space if you can’t sort your possessions into categories, Now, this might sound easy, but for people with a serious collecting and cluttering problem, this process can be quite stressful. Often, it’s because they’re worried that they might make a mistake and put something in the wrong category. Also, because everything is of equal importance when you have a serious collecting and cluttering problem, sorting forces you to decide what is important and less important. This is new territory for some people. To sort, label three boxes Very Important, Important, and Not at All Important. Now, sort possessions into one of those three boxes. Set aside the idea that you must discard an item. This isn’t about discarding. It’s about placing your possessions into categories. Focus on one small spot at a time. If you have a serious collecting and cluttering problem, you likely have a lot of stuff. Typically, people declutter here and there, moving from one pile to the next. This means that you could work all, look at your living room, and think that you’ve accomplished nothing. This is demoralizing. Instead, focus on one small spot and stay on that spot for as long as you plan to declutter. If you have a Hula Hoop, place it over the area you wish to focus on and only deal with the items in the hoop. Manage distraction. Decluttering isn’t a lot of fun. In fact, it’s boring. If you’re easily bored then you can expect to get distracted when you declutter. To manage distraction, try a couple of things. First, use a timer on a lanyard that you can wear around your neck. Wearing the timer around your neck prevents you from wandering away from the timer as you declutter an area. When you begin to declutter, set the timer for 10 minutes. When the timer sounds, ask yourself, “Am I working on what I decided to work on when I set the timer?” If the answer is yes, reset the timer for another 10 minutes and get back to work. If the answer is no, go back to the spot and try again. Another way to manage distraction is to work for sort periods and then take attention breaks. Sorting and decluttering takes a lot of mental effort (not to mention physical effort). Work for a short period, say 20 minutes, and then give yourself a short break, say 5 minutes. Remember to set the timer for 5 minutes when you start your break. This will help you keep to short breaks. Last, if you’re decluttering an area – your sofa, for example – try covering with a bedsheet or drop cloth everything on the sofa, except the area on which you’re working. If you use the Hula Hoop idea, cover everything on the sofa but the Hula Hoop Develop decision rules. Decluttering involves many, many decisions. Not just deciding what to keep and what to discard, but deciding where and how you’ll store the things you decide to keep. Because it can be difficult for people with a serious collecting and cluttering problem to make decisions, decision rules can help. For example, consider these rules: “If it’s broken, then I’ll discard it.” “If I haven’t worn the item in a year, then I’ll give it away.” “If I don’t have enough space to store it, then I’ll give it away.” “If it’s dirty, I’ll either clean it today, or discard it today.” Write these rules on a big piece of butcher paper and tape it on the wall across from the area your clearing. When you have some trouble deciding what to do with an item, look at the decision rules and go through the questions. Decision rules can really help move along the decluttering process and save you time.
One Reason Why Your Workbooks Aren’t Working

A major challenge to using a mental health workbook is that we tend to make quick conclusions about how helpful a given exercise or tool will be.
Responding to Ambivalence in People Who Hoard

Ambivalence – and a great deal of it – is a typical feature of hoarding disorder. Given the considerable ambivalence of most clients with this condition, clinicians want to take care to avoid inadvertently shutting down the client’s motivation to work on the problem. Here are typical ways clinicians shut down motivation when treating hoarding disorder.
Handling Poor Treatment Response with Adolescents

Psychotherapy with adolescents is a difficult proposition. Research suggests that adolescents do not do as well as adults in psychotherapy and that they tend to dropout or refuse treatment more often. The cognitive-behavioral treatment for obsessive-compulsive disorder (OCD) is no exception.
How Families Can Help a Love One Who Hoards
If your loved one suffers from hoarding disorder, you’ve likely tried to help. You may have offered to clean her home or to hire someone to do it. You may have suggested that your loved one meet with a therapist or talk about the problem with a doctor; you may have purchased books on the topic and given them to your loved one to read, or searched for hours on the Internet for resources that could help—and, to all these efforts, your loved one has said no. Your loved one’s refusal to accept help, or even to admit that there’s a problem, is perhaps the most frustrating and demoralizing aspect of the problem for family members. The first step toward helping your loved one is to understand why he or she is reluctant to accept help from you or perhaps anyone. Why They Refuse Help Although some with the problem do see that the clutter is excessive and that their living conditions are unsafe and uncomfortable, many do not. Many people who hoard resist or avoid treatment or help. They appear baffled by family members’ reactions to the clutter, and are oblivious to the risks and discomfort that come with living with too many things. Typically, these people are older and have suffered from the problem of hoarding disorder for years, often decades, and live in very dilapidated and unsafe conditions. They tend to minimize the severity of the situation with comments such as “My house isn’t that messy,” and show little awareness of the problem, even though they may be smart and rational in other ways. Typically, when these people do accept help, it’s because others have forced it upon them. Even when refusing help may mean eviction, some people still say no. Poor insight, disagreement about how to solve the problem, fear, hopelessness, resentment and mistrust, and personal values are some of the reasons your loved one refuses help. Poor Insight. Clinicians describe people who don’t appear to recognize that their thoughts or behaviors are excessive or irrational as having poor or low insight. The adult daughter of a woman who had hoarded for thirty years described her mother in this way, “My mother’s a very bright woman—she’s a Phi Beta Kappa, for God’s sake—but when it comes to her stuff, it’s as if she has a hole in her brain. She just doesn’t get it.” Hoarding disorder appears to be a condition of low insight, as are other psychiatric conditions, such as psychotic disorders (particularly schizophrenia), anorexia nervosa, or body dysmorphic disorder. Because low insight prevents people who hoard from perceiving that they have a problem, they don’t believe they need help. However, this isn’t to say that people who hoard never feel distressed or uncomfortable. Many do. Most often, however, they’re distressed only when other people either prevent them from saving more things or when public health officials force them to either clear out their possessions or face eviction. The simple fact of the matter is this: people don’t see that there’s a problem unless they feel distressed by it. That’s why you’re more eager to solve the hoarding problem than your loved one: the hoarding problem distresses you more than it does your loved one, and no amount of reasoning, cajoling, arguing, or threatening is likely to change that. Disagreement about the Best Solution. Sometimes people who hoard admit that they have a problem, but don’t see it the same way family members do. Your loved one may tell you that it’s not that bad or that it really doesn’t interfere with his life all that much, and certainly your loved one will scoff at the idea of seeking help or treatment for the problem. Instead, your loved one will suggest that you help him find more space to store his acquisitions or to remove a few things from his home when what he needs is a much larger clear-out intervention. Disagreement about the best solution to the hoarding problem often leads to endless and circular discussions about what to do. At first, both the family members and the person who hoards believe that they’re working on the problem. Only later, after many arguments and hurt feelings do they realize that they’re digging in rather than digging out. Fear. Often people who hoard refuse help because they’re afraid. They may fear discovery and eviction or that others will come into their homes and, in a frenzy of helping, clear out all of their possessions. Due to the fear of discovery they don’t permit people into their homes who could repair the refrigerator, stove, or leaky toilet. If they rent, they never complain to the landlord about a broken pipe or furnace, because they fear the landlord will want to come into the apartment to have a look around. They know at some level that if others discover the hoarding problem, they’ll suggest, perhaps insist, that something be done. This fear isn’t unreasonable, because if the problem is discovered, that discovery may lead authorities to remove all or most of the possessions or to even evict your loved one from his home. Because they fear discovery, people who hoard often live in dangerous and unhealthy homes. If you have a family member who hoards, you may fear discovery of the problem as well. If the landlord evicts your loved one, where will he go? You may not be able to afford alternative housing for your loved one, such as a retirement or assisted-living facility. Even if you can afford alternative housing for your loved one, you may worry that the facility’s managers won’t accept your loved one if they know that she has a hoarding problem. If an assisted-care facility refuses your loved one, would you want him to live with you, knowing that the hoarding problem would come as well? For these reasons, family members will sometimes help their loved one keep the secret, not just because they themselves are ashamed about the problem
Perfectionism: When setting high standards backfires
Striving to do well is a positive attribute as long as there are no negative consequences for doing so. A healthy desire to excel and achieve high standards is one thing. Perfectionism, though, can be problematic if you evaluate yourself based on self-imposed, highly demanding standards, especially in areas of life that are important to you. Even if you complete a task quite well, you may still criticize yourself for not doing it quickly enough or for not getting it done right the first time. If your self-worth is based on your ability to achieve perfect standards, you are likely to evaluate yourself as inadequate and suffer from ongoing self-criticism. You may compare yourself to others and believe that you aren’t as capable as they are or that they are evaluating you negatively because you can’t live up to your standards of perfectionism. These comparisons can lead to feeling down about yourself and your accomplishments. What may initially seem like a healthy desire to do an excellent job turns into a problem, sometimes a big problem. Setting perfectionistic standards can lead to spending an excessive amount of time on work projects or even avoiding them for as long as possible due to the burden of always trying to do a “perfect” job or fearing that you’ll fail to achieve your perfectionistic standards. The costs of striving for perfectionism can be high. Your anxiety about being perfect may lead to making more mistakes. The excessive time you spend on tasks or avoiding tasks may interfere with completing tasks in a timely manner. Problems with perfectionism can interfere with your quality of life in many ways, including maintaining job satisfaction and spending quality time with loved ones and friends. They can contribute to symptoms of anxiety or depression. Accepting that you are not perfect (i.e., you are human like everyone else!) and that striving to achieve perfectionism paradoxically often works against achieving your desired goals is a giant step toward being free to do your best work without the burden of inflexible, self-imposed standards that often get in your way. Looking at the costs and benefits of striving for perfectionism, completing experiments to test out your beliefs about the consequences of not being perfect, and accepting uncertainty about making mistakes while focusing on the task at hand, are strategies that can help you break free from the constraints of self-imposed perfectionism standards and the negative consequences that often follow.
Two Willingness Strategies in Cognitive-Behavior Therapy
Although cognitive-behavior therapy helps many clients with anxiety disorders, the exposure tasks, which are central to overcoming an anxiety disorder, are not easy. Because exposure to anxiety-evoking situations is difficult, attending to your client’s willingness throughout treatment is essential to a good outcome. Here are two standard cognitive-behavioral strategies to enhance willingness.
Enhancing Adherence with Bibliotherapy
Self-help reading is often assigned as an extra-therapy activity and, like any homework assignment, thoughtful planning on the part of the therapist can mean the difference between a homework assignment that is completed or not. The following guidelines can improve the likelihood that clients will understand and complete self-help readings. Never assign a self-help reading that you haven’t read first. In these busy times, it’s understandable that therapists might recommend a book to a client based on an endorsement from a colleague or another client or after only a brief review of the book. There are a number of good reasons why it is essential that therapists read the self-materials they have assigned. Not all self-help materials are helpful. Sometimes, a self-help book will reinforce a problematic view the client holds that the therapist is working very hard to correct. For example, many self-help books emphasize change when acceptance is a better strategy for many clients. This is particularly true of individuals with chronic conditions such as dysthymia in which their efforts to “feel happy” only aggravates their condition as they become self-critical when they are unable to meet this unrealistic expectation. Therapists who read self-help books before they assign them can discuss with their clients the importance of taking a balanced view toward their condition and to not set unrealistic expectations. Often, after reading self-help material, clients will have questions or will want clarification about a point. Not only is it embarrassing for the therapist to say, “Where does it say that,” and reach for the book but it decreases the likelihood that clients will take self-help readings seriously: if the therapist hasn’t taken the time to read it, how useful can it be? Prescribe specific self-reading assignments rather than leaving to the client the decision of what to read and when. I have found prescribing specific chapters or pages in a self-help book more useful than suggesting clients read a book without any guidance as to where to begin or on what to focus. This approach is particularly helpful for anxious or indecisive clients who may need added encouragement and structure. Therapists can offer several choices of what to read and prioritize which chapters to read first, then second, and so on. It helps to write down dates and times when the reading is to be done, particularly for disorganized clients or those who have trouble following through with tasks. Clients may be more likely to read self-help materials if they believe that the readings have been individualized to their particular needs. Review with clients the table of contents of the prescribed book and discuss which chapters are relevant to them. I recommend that therapists predict that anxious clients may become anxious as they read the self-help materials, “Joyce, as you read about panic attacks you might notice yourself feeling a little anxious. This often happens to anxious clients and, in fact, it’s good practice for you because it’s important for you to become more comfortable with feeling anxious.” Then spend some time troubleshooting with clients what they might do if they become anxious so that they can continue the reading assignment. Present the rationale for each reading assignment and tie it to the client’s treatment goals. Clients are more likely to read self-help materials if they understand the reason for doing it. Goldfried and Davison (Holt, Rinehart and Winston, 1976) noted that presenting clients with a general rationale for treatment as well as explaining the link between the client’s and therapist’s definitions of treatment goals heightens the client’s view that therapeutic tasks, such as homework, are valid and credible. A rationale for a self-help reading assignment can be quite simple, “I think reading about the nature of anxiety and panic may help to correct some misunderstandings you have about panic attacks which may decrease the likelihood you’ll have one.” After providing a rationale for the self-help reading, check with clients whether they have accepted the rationale or not. Clients who reject a homework rationale may be less open to change, perhaps because they are hopeless about anything helping; because they have clear beliefs about what will and will not help them solve their problems that the therapist has not explored, or because they don’t understand the reason for doing it. Review the reading assignment each session. Careful inquiry about the client’s response to the self-help readings can improve adherence with future homework assignments as well as provide therapists with information that may assist treatment planning. For example, Jon, a 57-year old mechanic who had experienced a series of recent panic attacks agreed to read the first two chapters of a self-help book on panic. When his therapist asked Jon for feedback about the reading, he reported that the section on medical disorders with panic-like symptoms was particularly upsetting. Jon believed that he might be suffering from Meniere’s disease, a common disorder of the inner ear. Although Jon had been cleared medically, Jon’s therapist thought it prudent to discuss this information with Jon’s physician. Jon was then referred for an additional medical workup that confirmed an inner ear problem, although not Meniere’s disease. To check whether clients have understood what they have read, ask them to describe the main points of the readings as well as what was helpful or not helpful; ask them whether they have questions about the readings, and ask them whether they found anything to be upsetting or off putting. A self-help book can help many clients, if they read it. The challenge of therapists is to help their clients read what they have agreed to read and thereby learn what their therapists hope they will learn. I’ve presented four guidelines that therapists can follow to get self-help reading assignments off to a good start. Try them and see what you think.